Disorders of Consciousness (DoC) Rehabilitation: Introductory Strategies for Success

The rehabilitation of people with disorders of consciousness (DoC) poses unique challenges for clinicians. Due to their severe level of functional impairment, which cannot be treated using traditional rehabilitation techniques, patients benefit from a specialized approach to treatment.
The goal of this article is to provide clinicians with strategies to create individualized treatment plans designed to meet the unique needs of these patients.
What Causes Disorders of Consciousness?
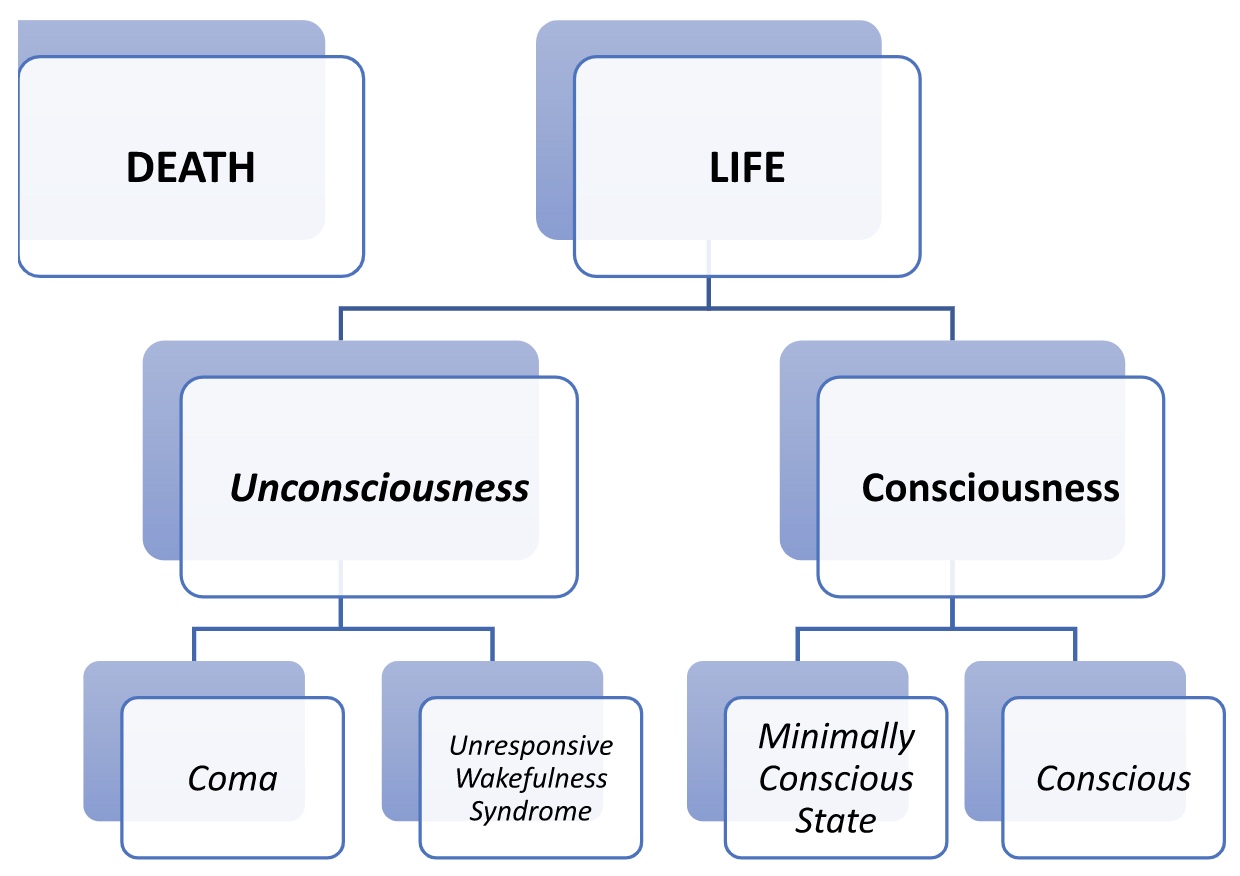
DoC are states in which consciousness has been affected by damage to the brain. Consciousness is defined by both arousal and awareness, as highlighted below.
| Arousal | Awareness |
|---|---|
|
|
Causes of DoC include congenital conditions, birth trauma, or acquired brain injury (traumatic and non-traumatic injuries). Disordered consciousness can also have reversible causes, including:
- Understimulation and undermobilization
- Disrupted sleep-wake cycles
- Sedating medications
- Concurrent medical conditions such as hypoxemia, infection, or metabolic abnormalities
- Neuroendocrine abnormalities
- Seizures
- Intracranial abnormalities such as hydrocephalus or subdural hygromas
The Three Types of DoC
DoC are diagnosed based on specific neurobehavioral functions, including:
Coma
Rancho Los Amigos Level I: No response
Coma is defined by lack of arousal and awareness. Characteristics of a person in a comatose state include:
- Inability to voluntarily open the eyes
- Depressed brainstem reflexes
- Failure to respond to stimuli
- Irregular breathing
- Absent sleep-wake cycle
- No initiation of voluntary actions
Coma is usually a temporary state and typically lasts less than four weeks. Most people will progress from a coma into another state of unconsciousness (i.e., unresponsive wakefulness syndrome) or a state of consciousness (i.e., minimally conscious state).
Unresponsive Wakefulness Syndrome
Rancho Los Amigos Level II: Generalized Responses
Unresponsive wakefulness syndrome is defined by arousal, but there are no signs of awareness. Characteristics of a person in this state include:
- Eye opening
- Present brainstem reflexes
- Presence of a sleep-wake cycle
- Spontaneous, non-purposeful movements, facial expressions, and vocalizations
- Reflexive, generalized responses to stimuli
- Posture or withdrawing to pain
- Brief movement of eyes toward people or objects
- Mouth movement to oral stimulation, such as biting down on a toothbrush, coughing, or swallowing
Minimally Conscious State
Rancho Los Amigos Level III: Localized Response
A minimally conscious state is defined by clear, but minimal or inconsistent awareness. Characteristics of a person in a minimally conscious state include:
- Eye opening/being awake for longer periods of time
- Ability to visually track
- Purposeful interaction with their environment
- Ability to follow simple, one-step commands
- Ability to answer simple yes/no questions
- Localization to sound
A minimally conscious state can be temporary or permanent. A person may enter a minimally conscious state after being in a coma or unresponsive wakefulness state. Entering a minimally conscious state may be permanent or preclude recovery to full consciousness. The chart below shows these neurobehavioral functions in relation to consciousness.
DoC Rehabilitation
When addressing consciousness and communication, accurately assess the current level of consciousness using assessments like the Coma Recovery Scale-Revised (CRS-R) and address and/or take into account reversible causes of impaired consciousness.
Trial interventions to enhance the level of consciousness and promote responsiveness, including multi-modal sensory stimulation (for example, the “coma stim” program) via graded auditory, olfactory, visual, vestibular, tactile, kinesthetic, and oral-motor stimuli. Closely monitor for physical and physiological changes and document observations thoroughly.
If appropriate, establish a system of communication. Ask questions or provide choices in a “field of two,” for example yes/no. Maintain environmental control (for example, by keeping the room calm and quiet). Identify yourself and orient the patient frequently. Explain what you are about to do prior to any intervention. For example, when moving the patient’s arm, clearly state, “I’m going to move your arm.”
Talk in a normal, clear tone of voice. Keep comments and questions short and simple. Say, for example, “Look at me,” instead of, “Can you turn your head toward me?” When addressing physical impairments, consider:
- Minimizing restrictions in range of motion
- Contracture management and prevention
- Identifying and augmenting residual voluntary movement
- Intensive mobilization and environmental enrichment
- Preventing and managing secondary medical complications
- Optimizing basic bodily functions, such as respiration, nutrition, elimination, and skin integrity
Throughout the continuum of care, provide your patients’ family caregivers with education, training, and support, as well as extensive discharge preparation to ensure they are ready for the challenges ahead. MedBridge offers many caregiver courses that teach caregivers how to assess symptoms, manage pain, and assist in daily living.
Ethics
Few patients in a DoC state have advanced directives in place on continued life-sustaining therapy. Typically, approval must be obtained from family or legal representatives in any treatment decisions, including withdrawal of care. DoC treatment requires significant healthcare dollars and resources, including extensive maintenance/treatment in intensive care units (ICUs) or step-down units (SDUs). Some argue that resources shouldn’t be used by patients who seem to have little or nothing to gain from them.
Though there is controversy surrounding the treatment of DoC, some studies have provided evidence indicating the reversibility of DoC and demonstrate that patients may be aware despite clinical unresponsiveness.These recent findings could have a major impact on ethical questions and concerns surrounding DoC treatment.
- Eapen, B. C. & Cifu, D. X. (2018). Rehabilitation after traumatic brain injury. Elsevier.
- Lin, K. & Wroten, M. (2022). Ranchos Los Amigos. StatPearls.
- Reyst, H. & Brain Injury Association of America. (2016). The essential brain injury guide (Edition 5.0). Brain Injury Association of America.







