Vectors: What Are They and What Are They For?

As rehabilitation professionals, we have a high level of skill in prescribing exercises that challenge our patients, especially when it comes to function. As we strive to make an exercise more functional, we inevitably run into a challenge—the more complex we make an exercise, the more likely it will be performed incorrectly.
Take, for example, a patient who lacks rotator cuff strength. Your goal is to progress their resistance band rotator cuff exercise from the elbow at their side to the elbow at their shoulder height. You prescribe the exercise with a raised elbow, but they cannot perform it correctly. Their shoulder blade keeps rounding forward as they pull on the band. You try to cue them to perform the correct movement, but you are unable to change their movement errors.
What do you do? Do you reduce the resistance of the band? Do you regress the exercise back to the elbow at their side? Or is there a way that you can facilitate scapular control while their arm is overhead?
As we increase the challenge of an exercise, form typically starts to break down. We can no longer target the specific muscles we had intended, and we often just prescribe a lower-level exercise that the patient can perform correctly. But regressing exercises that are performed incorrectly is not always the solution. We may be able to perform a higher-level exercise with proper form by improving selective muscle recruitment and motor control through varied vectors.
What Are Vectors?
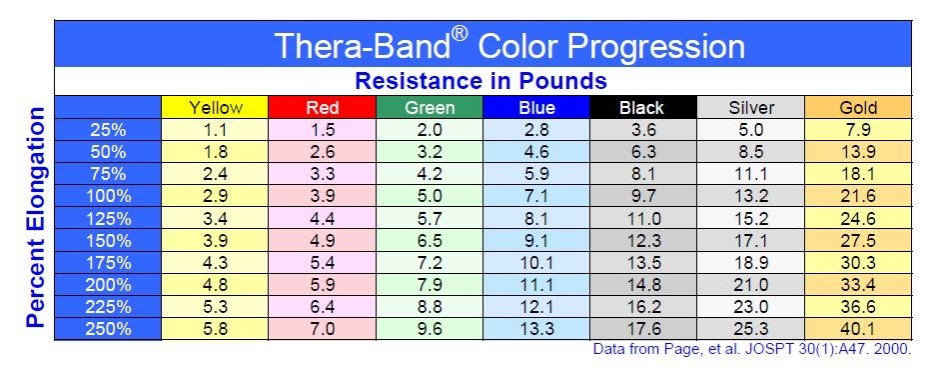
A vector is any load with a magnitude (a loaded pull or push) and a direction (where that pull or push is coming from or going to). All force you apply, and all resistance you provide—be it manually or with weights and bands—has a magnitude. A 10-pound weight provides magnitude, as does, for example, a fully elongated green Thera-Band (also about 10 pounds).
Direction is, quite simply, the direction in which the magnitude pulls. For a dumbbell, this is always downward. For a resistance band, this is wherever the band is anchored.
Types of Vectors
Vectors can help achieve specific joint or body positions, or specific muscle recruitment behaviors, and reduce compensations. Vectors can achieve this by providing resistance (wherein the patient moves against the vector), assistance (wherein the patient moves with the vector), or a combination of the two.
Vector of Resistance
A “vector of resistance” uses a directional load to help a patient generate specific joint or body position with specific muscle engagement. Vectors of resistance can help train a strong muscle to manage a specific movement. For example, the video below shows a vector of resistance challenging the scapular depressors to resist against the upward pull.
Vector of Assistance
A “vector of assistance” also uses a directional load to help a patient achieve a specific joint position during a movement. Vectors of assistance can help a weak muscle get stronger in a specific position or posture. For example, the video below shows a vector of assistance helping to elevate the scapula (indirectly through the distal humerus).
Combining Vectors
While vectors of resistance and assistance can be great training tools when used individually, you can combine them into “dual vectors” to train joints, muscles, or body regions to behave simultaneously in very specific ways. This takes advantage of a concept known as “regional interdependence”.
What is Regional Interdependence?
Regional interdependence, alluded to in all but name as describing the “kinetic chain”1 is effectively a mechanical and/or neurophysiological link between different regions of the body, whereby dysfunction (or treatment) of one region can significantly impact pain or function of another remote region.2
In effect, regional interdependence refers to the way that the behavior of one part of the body (i.e. the elbow or knee) depends on the function of another part (i.e. the scapula or hip). Optimizing the function of one region, such as the shoulder girdle or hip, can improve the behavior of another region, such as the elbow or knee.
Dual Vectors
A dual-vector setup uses two vectors to simultaneously influence the behavior of two body regions. For instance, in the example of rotator cuff strengthening in an individual with poor scapular control the patient’s primary vector is the resistance band they were using to strengthen their rotator cuff.
However, an additional vector, in this case another resistance band, could be looped around their shoulder blade to facilitate proper scapular position. It can be added as a vector of resistance (wherein the band is in front of the patient, and they retract into it) or assistance (wherein the band is behind the patient and passively pulls them into scapular retraction), or a combination of the two.
See below for an example of a high elbow rotator cuff exercise. The primary vector of resistance is into humeral external rotation whereas the secondary vector of resistance is into scapular retraction.

There are many additional ways to incorporate vectors during the same rotator cuff exercise with patients who show movement faults. For example, what if the patient exhibited excessive scapular retraction/depression or excessive scapular elevation/protraction. How would you optimize their exercise performance and correct the movement errors by utilizing vectors?
Below is another example of utilizing dual vectors. One vector at the trunk and one at the hip can help improve the movement economy and efficacy of a tennis swing. There are dual vectors of resistance – at the trunk, and at the hip – to improve core muscle power and coordination during this movement.
Two vectors of assistance can be as well to improve mobility and joint positioning. For example, if a patient presents with a hypomobile talocrural joint that is limiting dorsiflexion, a primary vector of assistance can be used to traction the joint while a secondary vector of assistance can be used to assist in open kinetic chain dorsiflexion.
In another example, dual vectors of resistance at the cervical spine and elbow help train concurrent control of craniocervical flexion and elbow extension during a sport-specific movement. In this case, it is during a rock-climbing belay, where a climbing partner on the ground is in overall cervical extension to look up at a climber on a rock face while performing elbow extension to manage the rope linking the two of them.
Specifically, this demonstrates how dual vectors do not need to be set up in obviously related ways. Rather, the dual vector setup relates overall to the related function of these two body regions.
When training specific strength, or activity-specific movement strength and quality, the setup of your resistance is key to achieving the specific desired outcome. Using and even combining vectors can help facilitate strengthening a weak muscle into the desired position or training an already-developed muscle to participate optimally in the desired movement. Thinking, and setting up, in terms of vectors can help clinicians achieve activity-specificity without sacrificing specific muscle development while minimizing compensations.
For more information on the use of vectors and other interventions, Jared offers a series of MedBridge courses on The Movement System and The Athlete Movement System.
- Steindler, A. “The Pathomechanics of the Sacrolumbar Junction.” Instr Course Lect., 1955, pp. 177–188.
- Sueki, D. G., Cleland, J. A., & Wainner, R. S. (2013). A regional interdependence model of musculoskeletal dysfunction: Research, mechanisms, and clinical implications. Journal of Manual & Manipulative Therapy, 21(2), 90–102. https://doi.org/10.1179/2042618612y.0000000027







