Medical and Behavioral Treatments for Poor UES Opening

When poor UES opening biomechanically contributes to a patient’s swallowing difficulty, we must perform a diagnostic assessment to establish the cause. Treatments for UES impairments depend on whether the disorder is isolated to the UES or a problem of traction, such as lack of hyoid movement.
Isolated to the UES
Disorders isolated to the UES itself – such as, disorders of relaxation or obstruction – typically require medical or surgical interventions, for example:
- Dilation
- Botulinum injection
- Cricopharyngeal myotomy
Causes of poor UES relaxation range from neurological impairments (e.g., rostral medullary lesions) to inflammatory myopathies. Various inflammatory conditions and chemoradiation therapy can create mechanical obstructions at the UES.
Problem of Traction
For many others, however, impaired UES opening can be attributed to weakness in the tongue or suprahyoid muscle complex. When the muscles that are responsible for hyoid excursion fail to adequately contract, the result is poor UES opening. Several exercises and maneuvers can be used to attack this traction problem:
- In a hard swallow maneuver, patients employ increased effort to drive the hyoid up and forward, thus improving UES opening.
- When the Mendelsohn maneuver is performed correctly, patients prolong elevation of the hyo-laryngeal complex, thus allowing the UES to remain open longer.
- The Shaker exercises are a series of isometric and isotonic head lift maneuvers intended to strengthen the suprahyoid muscle complex.
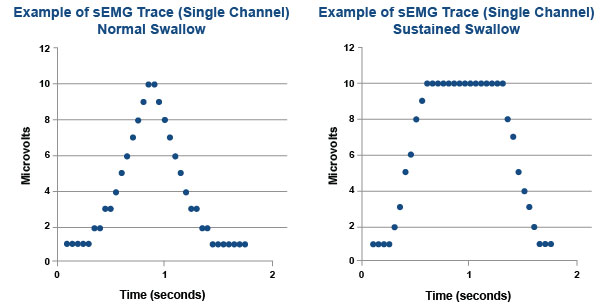
Surface electromyography (sEMG) biofeedback has succeeded in facilitating motor learning of new or unfamiliar movements. Relative to swallowing therapy, it was used to teach both hard swallows and the Mendelsohn maneuver. Patients can learn to alter the duration and amplitude of self-generated muscle activity by attending to either auditory signals or visual displays of data. Therapists establish thresholds of muscle activity and patients attempt to match the threshold. Displayed below, we see an example of an sEMG trace from a normal swallow compared to the trace from a successfully performed Mendelsohn maneuver. In the later trace, the individual was able to sustain their swallow at the established threshold.
Treatments vary greatly depending on the etiology of the UES opening impairment. Disorders isolated to the UES typically require medical or surgical interventions, whereas traction problems are amenable to exercises and maneuvers.
Next time you need to teach your patient a hard swallow or Mendelsohn maneuver, consider using an sEMG – if there’s one available in your practice – to facilitate their training.







